Designed to support flow-preserving radial hemostasis
SAPH (Suction Activated Patent Hemostasis) represents a non-circumferential compression, suction-based approach to radial closure that works with blood flow — not against it.
Developed by a leading interventional cardiologist, SAPH is designed to support hemostasis while maintaining arterial patency, contributing to smoother procedures, reduced post-procedure workload, and enhanced patient comfort.
By leveraging gentle, controlled suction rather than circumferential pressure, SAPH is engineered to help address the risk factors associated with radial artery occlusion (RAO) and preserve future access options.

The Compression Problem
Radial PCI may go perfectly for an hour. But the final step — closure — often introduces the greatest uncertainty.
That introduces variability in:
staff experience
monitoring frequency
compression adjustments
bleeding or occlusion risk
For the operator, the most delicate moment occurs after the procedure is complete.
Traditional compression devices require:
arterial compression
careful titration
constant monitoring
experienced staff
Once the patient leaves the procedure room, closure management shifts to the recovery area.
Closure in Practice
The most critical step begins after the physician leaves the room.
An expert discussion on variability in radial closure and post-procedure workflow.
Ronald Caputo, MD and David Cox, MD
Mechanism of Action
SAPH introduces a different approach to radial hemostasis.
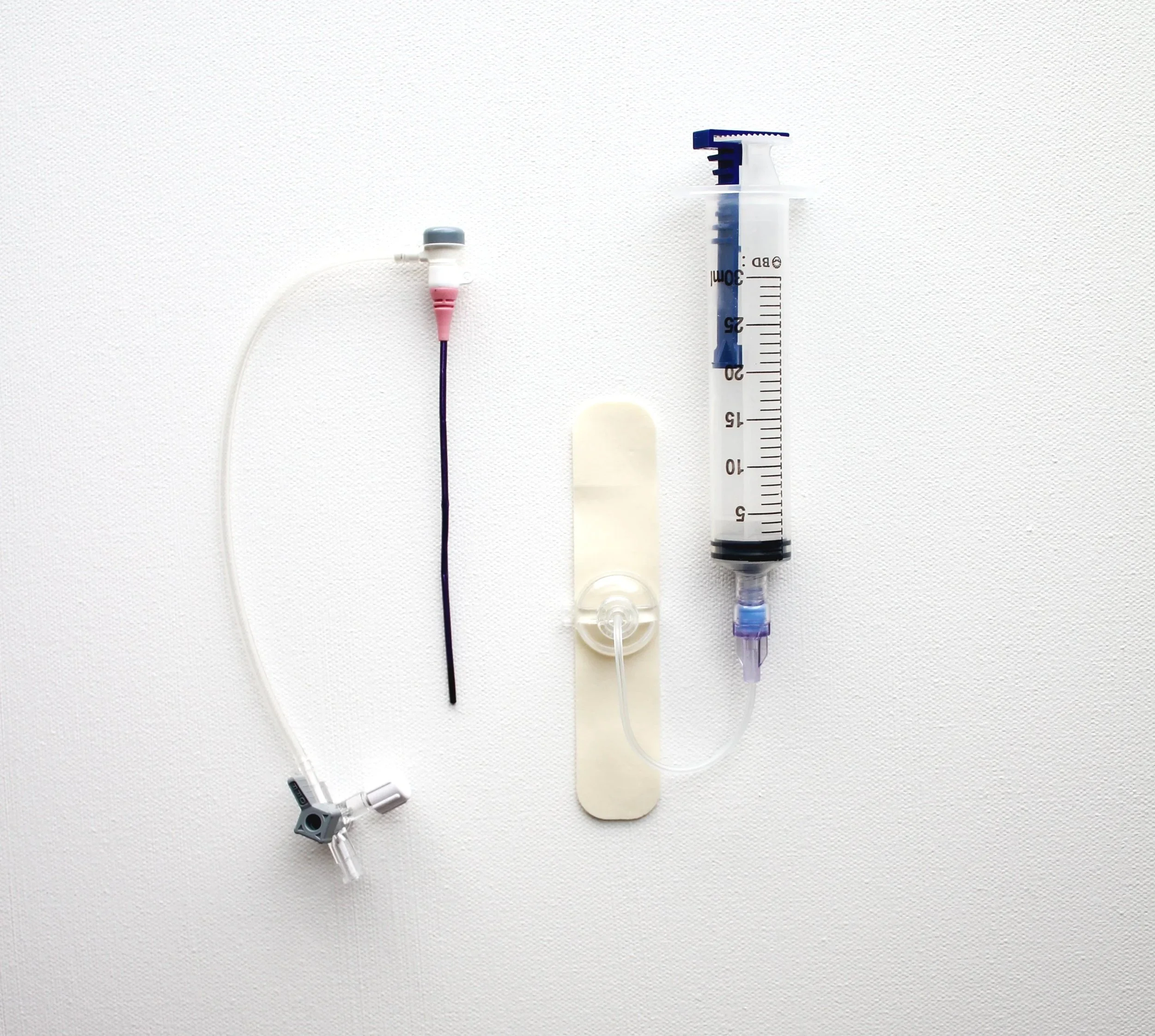
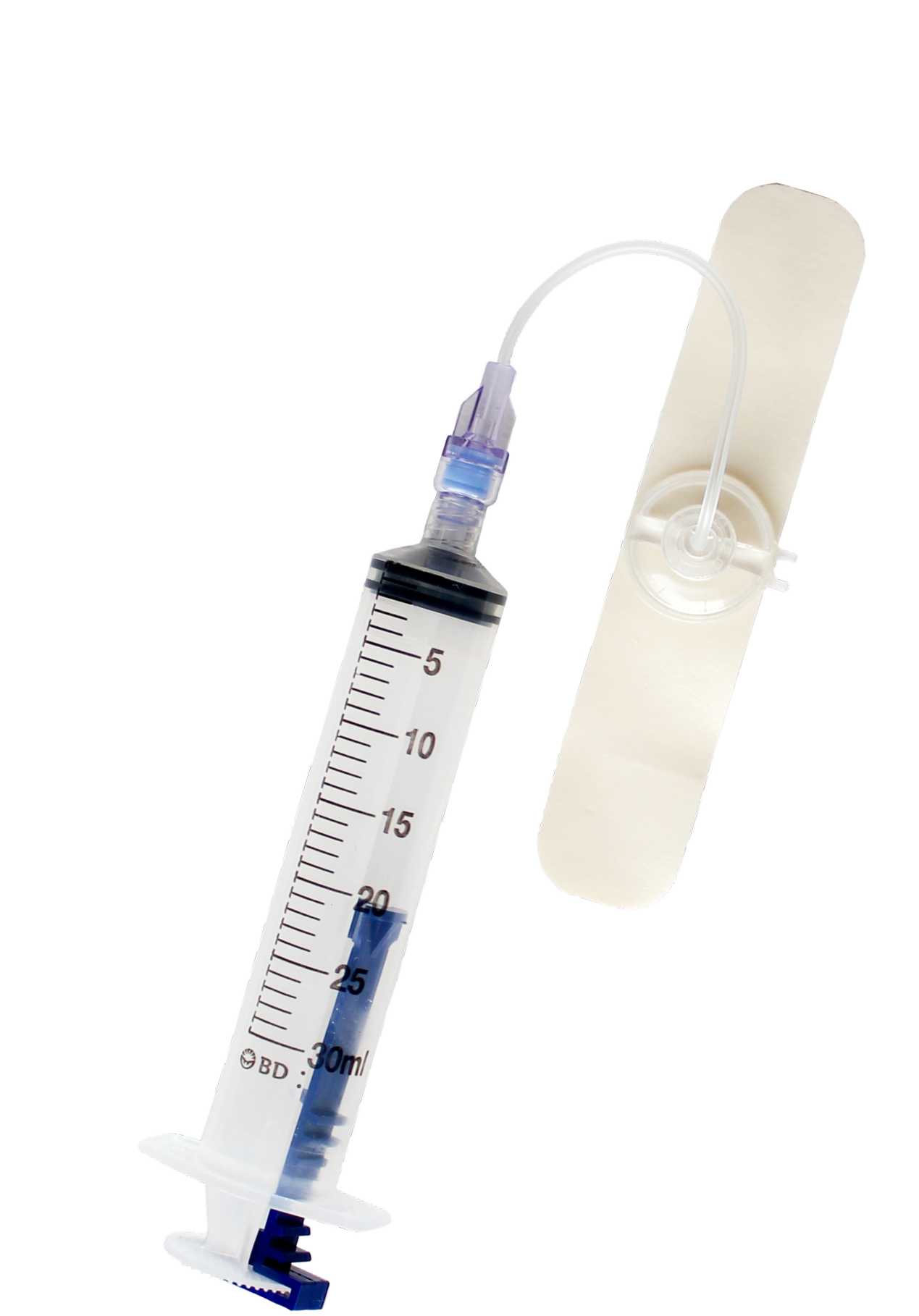
Suction Activated Patent Hemostasis
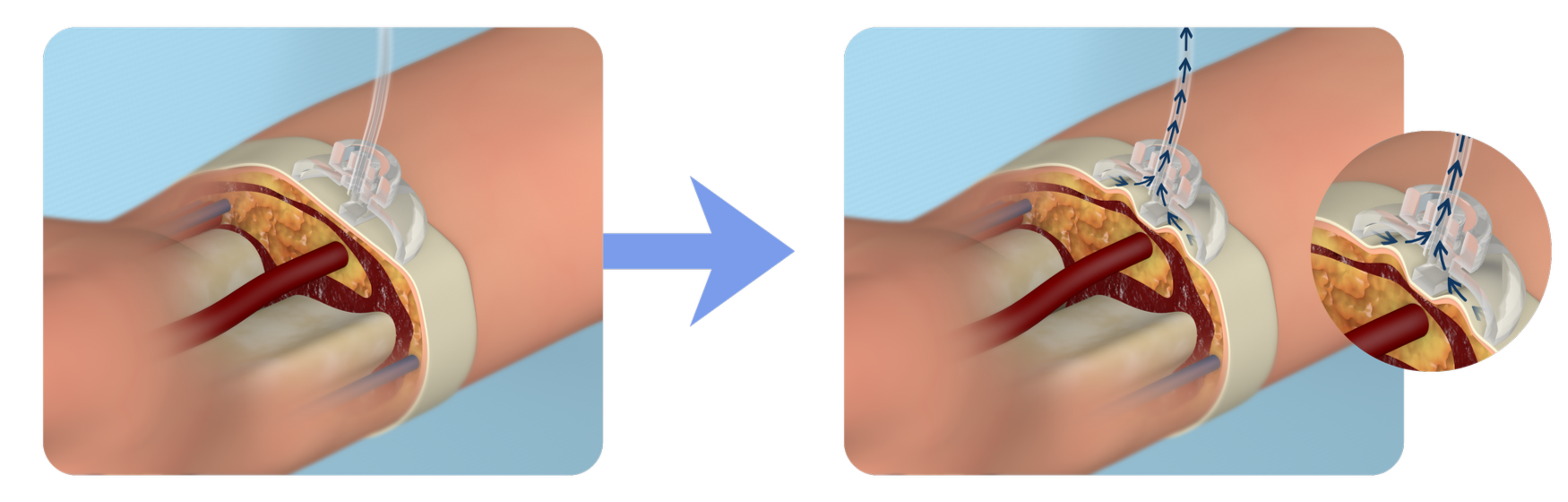
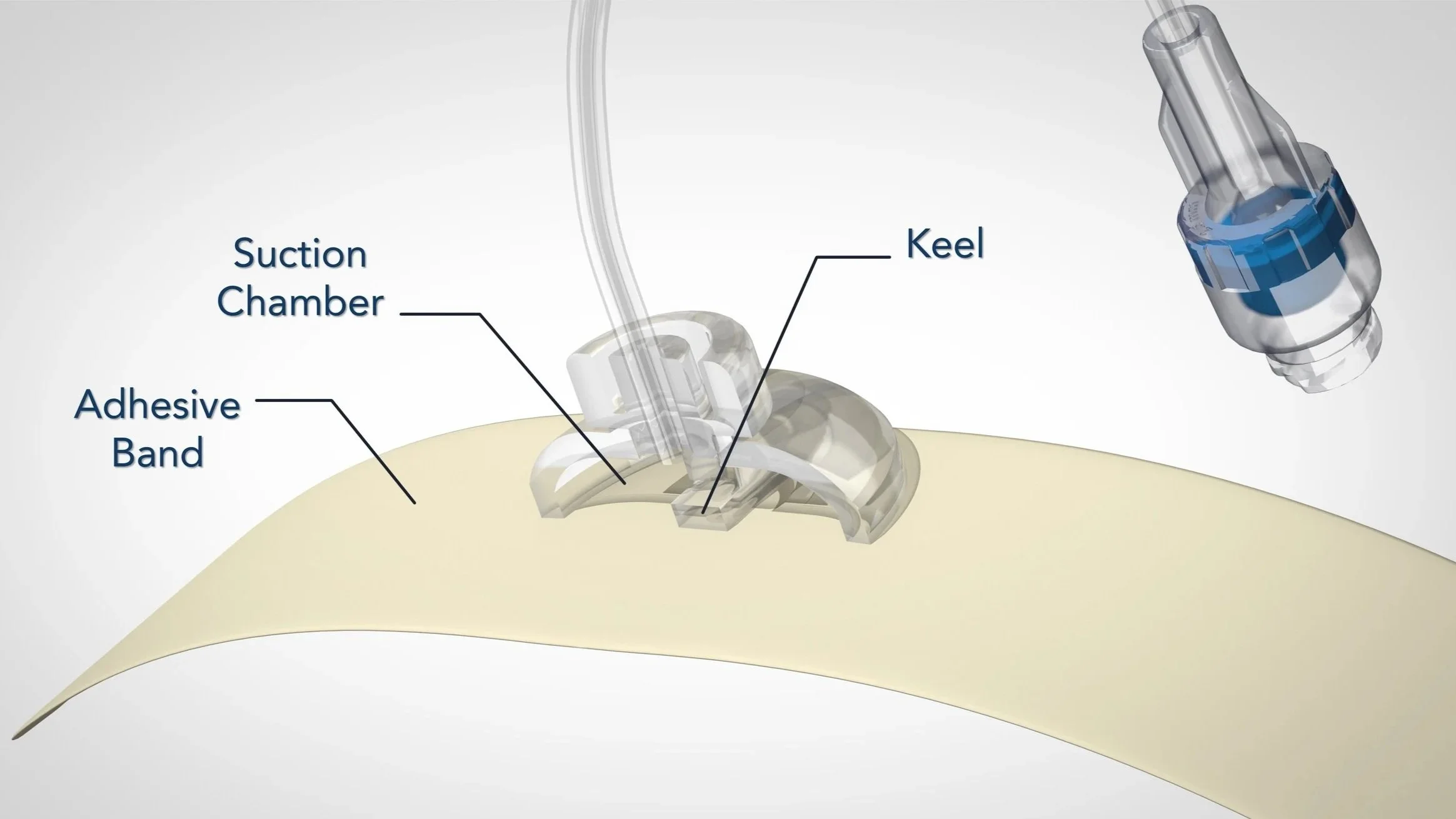
Instead of compressing the artery, SAPH uses controlled negative pressure to approximate the arteriotomy to a localized external seal.
Designed to Aid:
✓ Patent Hemostasis ✓ Flow ✓ Reduced need for staff adjustments
By supporting continued arterial flow during closure, the mechanism aligns with the principle of patent hemostasis, a widely recognized best practice in transradial procedures.
If radial access best practice emphasizes maintaining flow… Why does radial closure still depend on compressing the artery?
Radial Closure is Still a Compression Workflow
Compression-based closure typically requires:
staged deflation protocols
repeated nursing checks
pulse monitoring
bleeding management
reinflation cycles
Typical management time: 2-3 hours per patient
This creates significant recovery room workload and requires ongoing monitoring during the post-procedure period. [2]
SAPH Changes the Closure Workflow
Because the mechanism does not depend on titrated compression, the closure process is designed to become:
simpler to manage
less dependent on staff expertise
more predictable for recovery teams
Potential implications include:
reduced bedside intervention
more consistent hemostasis management
improved recovery workflow
Why This Matters
For Hospitals
Radial procedures represent millions of cases annually. [3]
Even modest reductions in recovery room workload can translate into:
Lower staffing pressure
Improved cath lab throughput
More predictable patient flow
For high-volume radial programs, improving closure workflow efficiency can have meaningful operational impact.
Strategically
Radial closure technology has remained largely unchanged for more than a decade.
This approach is intended to support flow-preserving radial hemostasis as an alternative approach.
Technologies that redefine procedural mechanisms often become highly valuable platforms within the cardiovascular ecosystem.
If maintaining arterial flow is best practice, shouldn’t radial closure evolve to support it?
About us
Transradial Technologies, Inc. is a medical device company focused on developing a novel, minimally invasive transradial vascular closure device.
Transradial Technologies, Inc. has worldwide and exclusive rights to the technology via an agreement with Transradial Holdings, Inc.